


 Sign Out
Sign Out



Children: Less than 50 kg weight 20 mg/kg daily may be increased in steps of 20 mg/kg every weeks to a maximum of 60 mg/kg daily.
More than 50 kg weight may be given the adult dose (see previously).
As monotherapy: 500 mg daily increased after 2 weeks to 1 g daily. Further increases may be made in steps of 500 mg every 2 weeks up to maximum of 3 g daily.
Oral solution: Monotherapy for adults and adolescents from 16 years of age: The recommended starting dose is 250 mg twice daily which should be increased to an initial therapeutic dose of 500 mg twice daily after two weeks. The dose can be further increased by 250 mg twice daily every two weeks depending upon the clinical response. The maximum dose is 1500 mg twice daily.
Add-on therapy for adults (18 years) and adolescents (12 to 17 years) weighing 50 kg or more: The initial therapeutic dose is 500 mg twice daily. This dose can be started on the first day of treatment.
Depending upon the clinical response and tolerability, the daily dose can be increased up to 1,500 mg twice daily. Dose changes can be made in 500 mg twice daily increases or decreases every two to four weeks.
Hepatic impairment: No dose adjustment is needed in patients with mild to moderate hepatic impairment. In patients with severe hepatic impairment, the creatinine clearance may underestimate the renal insufficiency. Therefore a 50% reduction of the daily maintenance dose is recommended when the creatinine clearance is <60 ml/min/1.73 m2.
Paediatric population: The physician should prescribe the most appropriate pharmaceutical form, presentation and strength according to weight and dose.
The safety and efficacy of Levetiracetam Oral Solution concentrate for solution for infusion in infants and children less than 4 years have not been established.
Monotherapy: The safety and efficacy of Levetiracetam Oral Solution in children and adolescents below 16 years as monotherapy treatment have not been established.
There are no data available.
Add-on therapy for infants aged from 6 to 23 months, children (2 to 11 years) and adolescents (12 to 17 years) weighing less than 50 kg: The initial therapeutic dose is 10 mg/kg twice daily.
Depending upon the clinical response and tolerability, the dose can be increased up to 30 mg/kg twice daily. Dose changes should not exceed increases or decreases of 10 mg/kg twice daily every two weeks. The lowest effective dose should be used.
Dose in children 50 kg or greater is the same as in adults.
Dose recommendations for infants from 6 months of age, children and adolescents: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdd-on therapy for infants from 1 month to less than 6 months.
The tablet formulation is not adapted for use in infants under the age of 6 months. The oral solution is the formulation to use in infants.
The initial therapeutic dose is 7 mg/kg twice daily.
Depending upon the clinical response and tolerability, the dose can be increased up to 21 mg/kg twice daily. Dose changes should not exceed increases or decreases of 7 mg/kg twice daily every two weeks. The lowest effective dose should be used.
Infants should start the treatment with Levetiracetam Oral Solution 100 mg/mL oral solution.
Dose recommendations for infants less than 6 months: See Table 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThis presentation should be prescribed for children older than 4 years, adolescents and adults.
A 150 mL bottle with graduated oral syringe containing up to 300 mg levetiracetam (corresponding to 3 ml) with a graduation every 0.1 mL (corresponding to 10 mg).
In order to ensure the accuracy of the dosing, the smaller bottle (150 mL) and syringe graduated from 0.1 to 3 mL per graduation of 0.1 mL should be prescribed for infants older than 6 months and young children.
A 150 mL bottle with graduated oral syringe containing up to 100 mg levetiracetam (corresponding to 1 mL) with a graduation every 0.05 mL (corresponding to 5 mg).
In order to ensure the accuracy of the dosing, the smaller bottle (150 mL) and syringe graduated from 0.05 to 1 mL per graduation of 0.05 mL should be prescribed for infants less than 6 months.
Method of administration oral solution: The oral solution may be diluted in a glass of water and may be taken with or without food. A graduated oral syringe, an adaptor for the syringe and instructions for use in the package leaflet are provided with Levetiracetam Oral Solution 100 mg/mL.
The daily dose is administered in two equally divided doses.
Julitam I.V.: Posology/frequency and duration of administration: The total daily dose and frequency of administration should be maintained. JULITAM IV concentrate for solution for infusion is for intravenous administration only.
There is no experience with administration of intravenous levetiracetam for longer period than 4 days.
Monotherapy: Adults and adolescents from 16 years of age: The recommended starting dose is 250 mg twice daily. The dose should be increased to an initial therapeutic dose of 500 mg twice daily after two weeks. The dose can be further increased by 250 mg twice daily every two weeks depending upon the clinical response. The maximum dose is 1500 mg twice daily.
Add-on therapy: Adults (≥18 years) and adolescents weighing 50 kg or more (12 to 17 years): The initial therapeutic dose is 500 mg twice daily. This dose can be started on the first day of treatment.
Depending upon the clinical response and tolerability, the daily dose can be increased up to 1500 mg twice daily. Dose changes can be made in 500 mg twice daily increases or decreases every 2 to 4 weeks.
Children aged 4 to 11 years and adolescents weighing less than 50 kg (12 to 17 years): The initial therapeutic dose is 10 mg/kg twice daily.
Depending upon the clinical response and tolerability, the daily dose can be increased up to 30 mg/kg twice daily. Dose changes should not exceed increases or decreases of 10 mg/kg twice daily every two weeks. The lowest effective dose should be used.
Dose in children 50 kg or greater is the same as in adults.
The physician should prescribe the most appropriate pharmaceutical form, presentation and strength according to weight and dose.
Dose recommendations for children and adolescents: See Table 3.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional information on special populations: Renal/Hepatic failure: The daily dose must be individualized according to renal function.
For adult patients, refer to the following table and adjust the dose as indicated. To use this dosing table, an estimate of the patient's creatinine clearance (CLcr) in ml/min is needed. The CLcr in ml/min may be estimated from serum creatinine (mg/dl) determination, for adults and adolescents weighting 50 kg or more, the following formula: See Equation 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThen CLcr is adjusted for body surface area (BSA) as follows: See Equation 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDosing adjustment for adult and adolescent patients weighing more than 50 kg with impaired renal function: See Table 4.
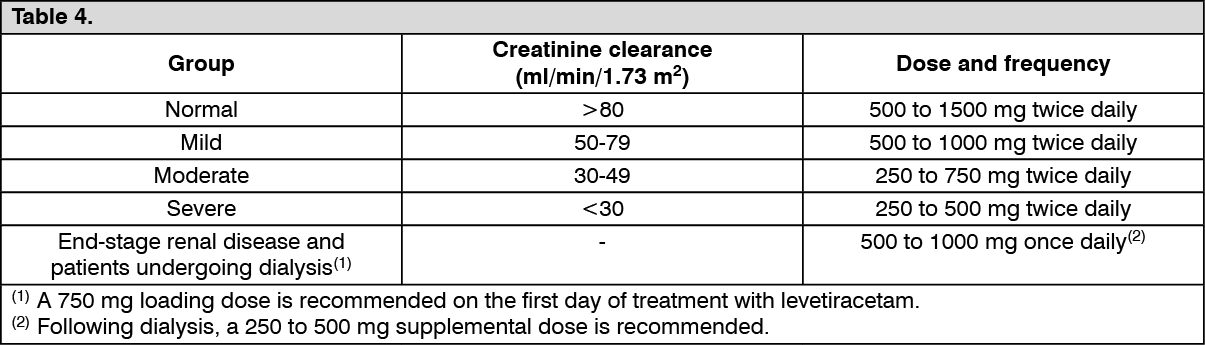 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor children with renal impairment, levetiracetam dose needs to be adjusted based on the renal function as levetiracetam clearance is related to renal function. This recommendation is based on a study in adult renally impaired patients.
The CLcr in ml/min/1.73 m2 may be estimated from serum creatinine (mg/dl) determination, for young adolescents and children, using the following formula (Schwartz formula): See Equation 3.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDosing adjustment for children and adolescents patients weighing less than 50 kg with impaired renal function: See Table 5.
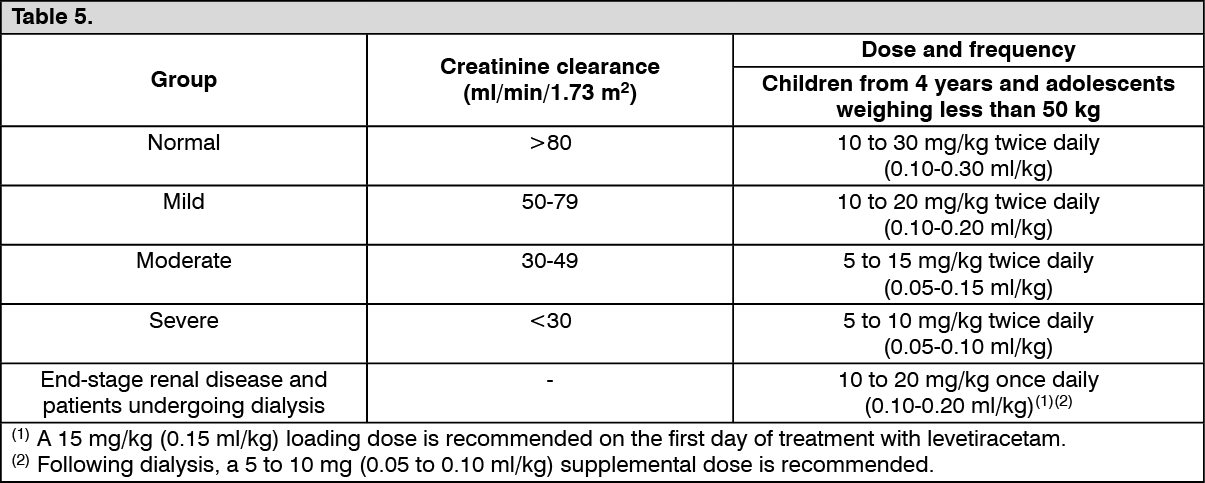 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNo dose adjustment is needed in patients with mild to moderate hepatic impairment. In patients with severe hepatic impairment, the creatinine clearance may underestimate the renal insufficiency. Therefore a 50% reduction of the daily maintenance dose is recommended when the creatinine clearance is <60 ml/min/1.73 m2.
Pediatric population: JULITAM I.V. concentrated solution for infusion is not recommended in children less than 4 years because of lack of sufficient data on safety and efficacy.
The efficacy and safety as a monotherapy treatment in children and adolescents under 16 years of age have not been established. Therefore, it is not used as monotherapy in children and adolescents under 16 years of age.
Geriatric population: Adjustment of the dose is recommended in elderly (65 years and older) patients with compromised renal function (see Renal/Hepatic failure as previously mentioned).
Method of Administration: Treatment can be initiated with either intravenous or oral administration. Conversion to or from oral to intravenous administration can be done directly without titration. JULITAM IV concentrate for solution for infusion is for intravenous administration only.
The recommended dose must be diluted in at least 100 ml of a compatible diluent an administered intravenously as a 15-minute intravenous infusion (for the preparation and information of compatibility, see Special precautions for disposal and other handling under Cautions for Usage).